
3rd BEACH Course - Session 2
How to deal with antibiotics and fluids (H Peperstraete)
If you think Pk/Pd on sick patients is challenging, imagine adding an ECMO circuit
Optimising drug dosing in patients receiving extracorporeal membrane oxygenation
Circuit factors
- LARGE surface area
- Drugs can be trapped
- Drugs can be released
Oxygenators (PMP): small losses of fentanyl and morphine
priming: ↑ circulating volume
Electrolytes, pH, temperature
Cristalloid- vs bloodprimed: affects proteinbinding, adsorption on tubings
Haemodilution: ↑volume of distribution (hydrophylic drugs)
ECMO & Increased Volume of distribution (Vd)
ECMO and drug clearance
- ♥: Initially↑ CO (fluids& inotropes), often myocardial depression => end organ failure
- Renal dysfunction: 32% in VV & 47% in VA
- Hepatic dysfunction
- RRT: 50%in VV& 41% in VA: importance of therapeutic drug monitoring
Fluids and ECMO
- SIRS
- Vascular permeability↑
- ECMO is preload dependent
- Large fluid amounts to prevent suction events
- Multiple drug infusions
- Large amounts of fluids
- Organ dysfunction
- AKI with oliguria or anuria, electrolyteand pH disturbances
Radiology of ECMO (K Nieboer)
The role of radiology in ECMO
- Pré ECMO imaging
- Important for decision making
- Baseline
- Before or soon after cannulation if possible
- Involve Radiology at an early stage where possible
- Done at the refferring centre if possible
- Per ECMO imaging
- Imaging modalities - X-ray, Ultrasound, CT scan
- Imaging findings / canula positions
- Haemodynamic changes important for CT imaging
- Complications
- CNS:
- Ischemic infarction (hypoexemia, acidosis, hypotension)
- Hemorrhage (anticoagulatio related
- Thoracic:
- Canula migration
- Effusions
- Pneumothorax
- Pulmonary embolism / Hemorrhage
- Others:
- Hemorrhage: intra / retroperitoneal / adrenal gland
- Hepatic infarction
- Arterial occlusions
- Deep venous thrombosis
- CNS:
Take home
- Communication and Planning
- Involve your (ICU) Radiologist
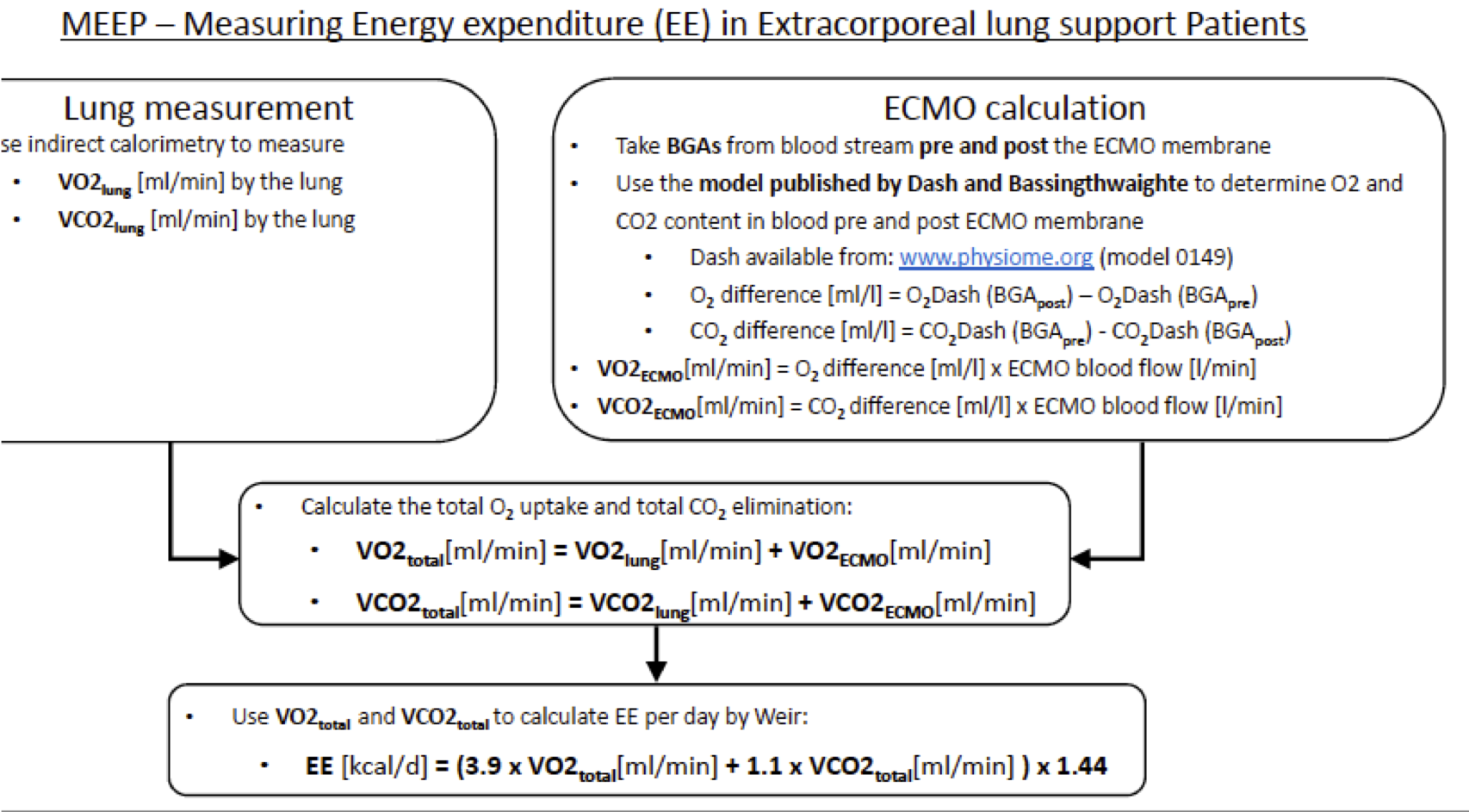
How to deal with nutrition? (E de Waele)
Very limited evidence - traditional mathematical formulas do not work.
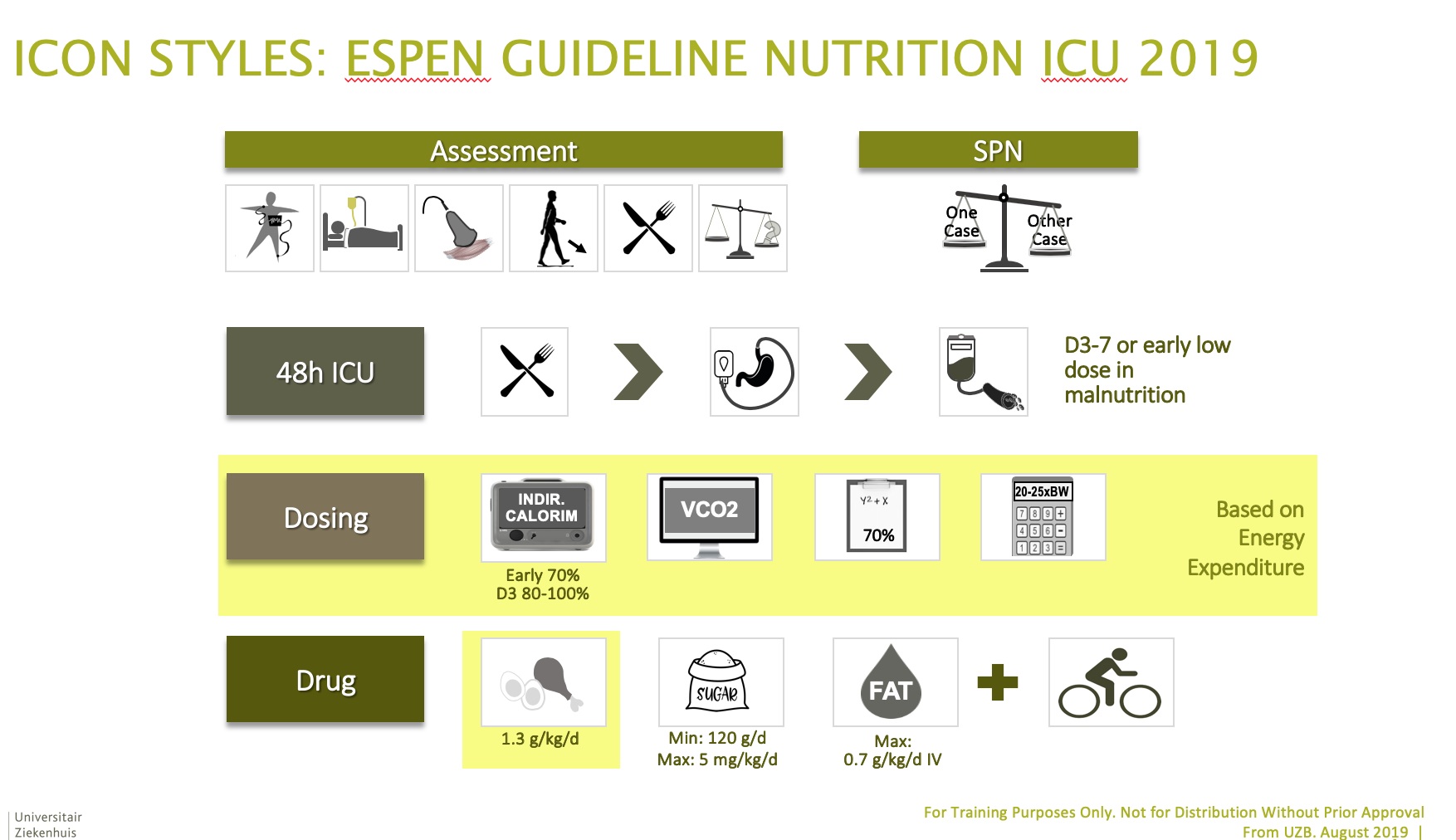
ESPEN guideline on clinical nutrition in the intensive care unit
Indirect calorimetry in nutritional therapy. A position paper by the ICALIC study group.
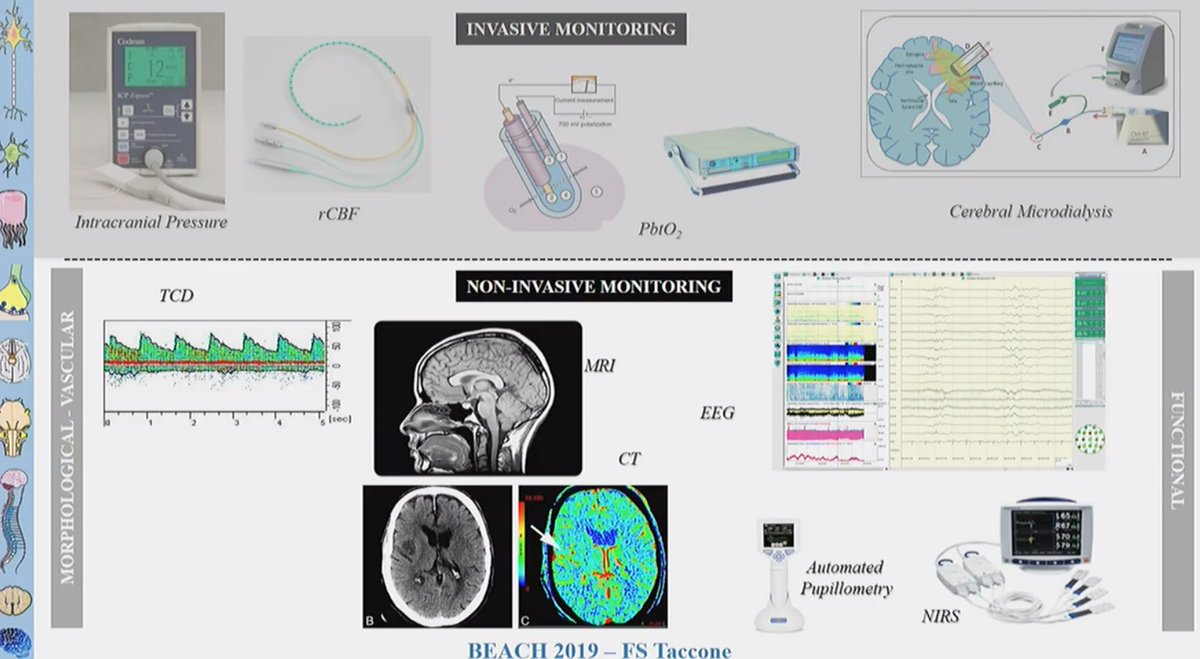
Neuro-monitoring during ECMO (F Taccone)
Acute Neurologic Complications During Extracorporeal Membrane Oxygenation: A Systematic Review.
Clinical examination -
… remains the best « tool » to evaluate the functional status, the severity of injury and assess prognosis in brain diseases
But is challenging in an ECMO patient (sedation, anoxic injury, encephalopathy)
So who should we monitor?
- Pre-ECMO characteristics
- Hypoxemia
- CVA
- Age
- Infection with neurological involvement (H1N1 – HIV?)
- Pre-ECMO Cardiac arrest
- On sedation / NMBAs
- Duration of MV - RRT
- Coagulation disorders – Use of anticoagulation
Neuromonitoring During Extracorporeal Membrane Oxygenation: A Systematic Review of the Literature.
CEREBRAL OXYGENATION
Near infrared spectroscopy is a non invasive technique which employes the use of near infrared wavelenghts emitted by sensor pads to evaluate regional oxygenation of the organ or tissue monitored. The difference in absorption of these wavelenghts by oxygenated and deoxigenated Hb is calculated, providing the clinician with information regarding the regional oxygen saturation (or saturation of cerebral tissue StcO2. NIRS monitoring is currently used during cardiac surgery, where it has also demostrated to be of great utility and where protocols of neuroprotection NIRS based have also been proposed, but there are only a few datas regarding its use during ECMO in adult population.
ELECTROENCEPHALOGRAPHY (EEG)
BRAIN BIOMARKERS
Biomarkers of mild traumatic brain injury in cerebrospinal fluid and blood
CONCLUSION
- Neurological complications during ECMO are frequent
- Neuro-monitoring may help in detecting brain “dysfunction” (perfusion, oxygenation or seizures)
- rSO2 and (c)EEG
- May help with prognosis