
3rd BEACH Course - Session 1
Indications and contraindications (S Bouchez)
The origins of ECMO, the story of the Lindberg pump - link
Indications for ECMO
- No absolute inidications
- Institute specific
- Multiple studies with variable outcomes
Advantages of ECMO
- Immediate improvement of hemodynamics
- Oxygenation & metabolic restauration
- Technical not difficult (relative)
- Bedside
- Compared to other options : $
Simplistically,
- Respiratory failure --> VV ECMO
- Circulatory failure --> VA ECMO
VV ECMO
- 80% mortality risk
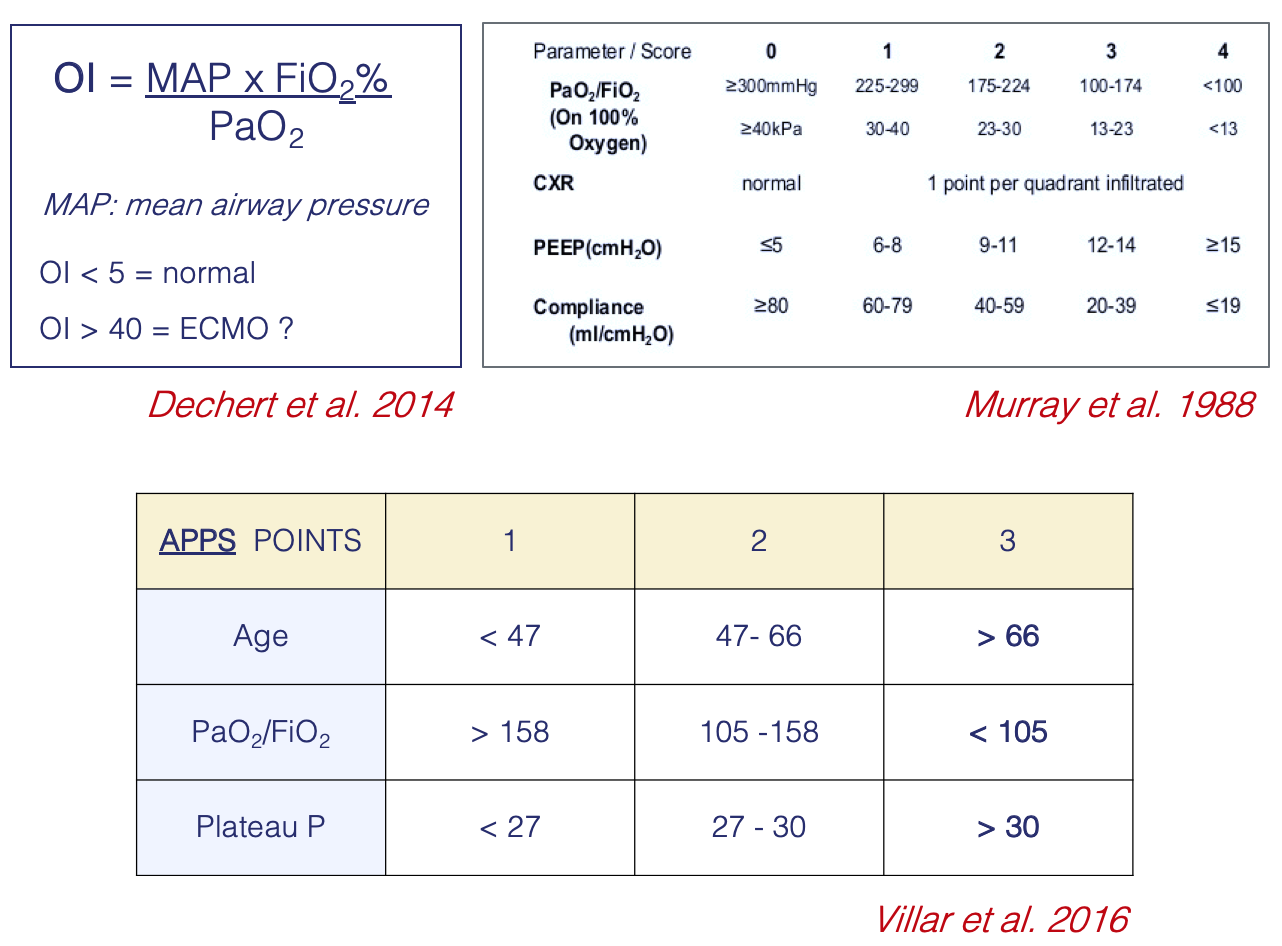
- PaO2/FiO2 < 100 on FiO2> 90%
- +/- Murray score 3-4, AOI >80, APSS 8
- despite optimal care for 6 hours or less
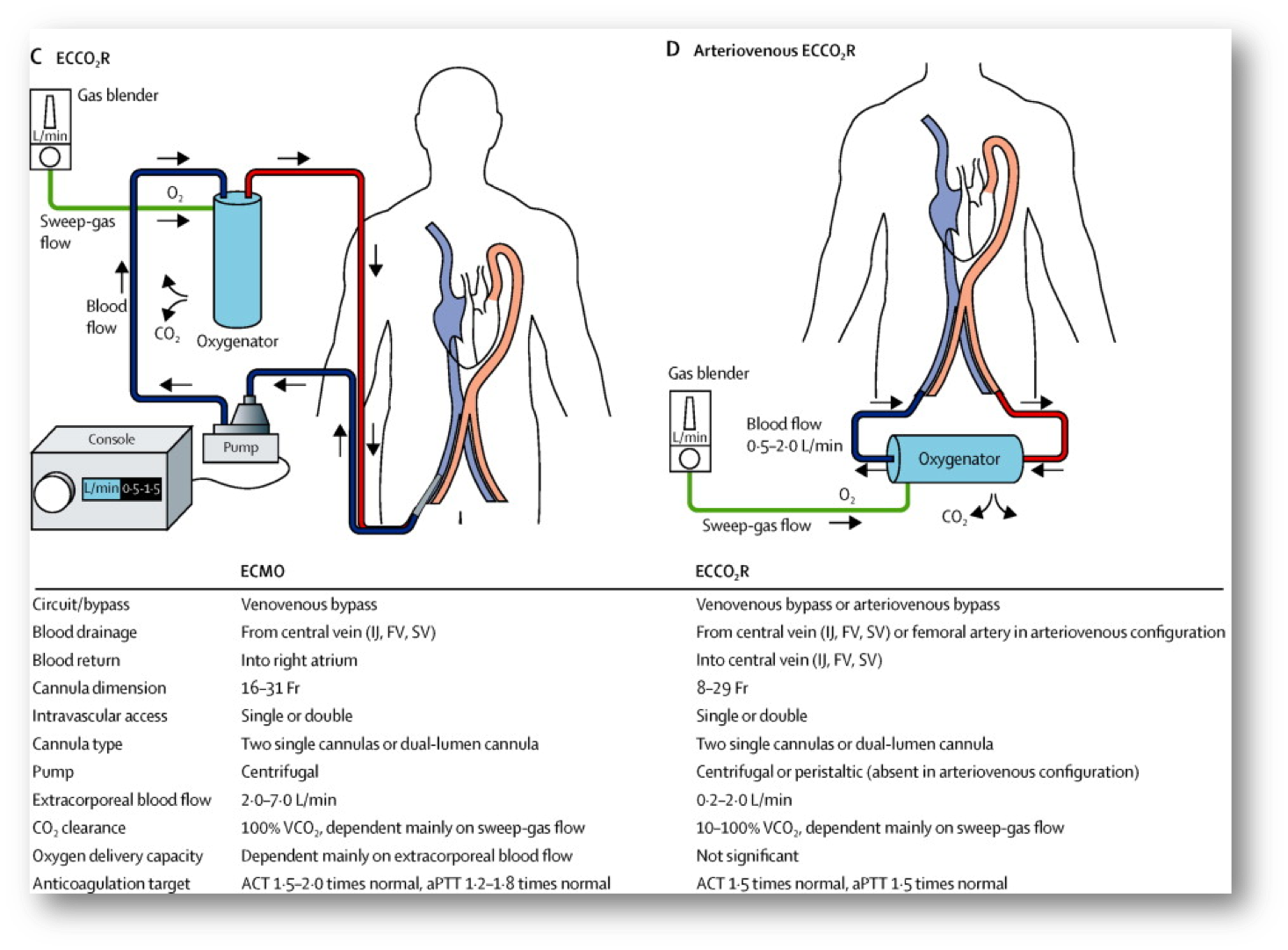
- CO2 retention
- despite high Pplat (> 30mmHg)
- Other
- Severe air leak syndromes
- Respiratory collapse ( blocked airways…)
- Surgery (trachea…)
VA ECMO
- Cardiogenic shock
- Acute coronary syndrome
- Myocarditis
- Pulmonary embolism
- Post-cardiotomy
- Periprocedural support
- PCI
- Surgery
- Sepsis (in some centers)
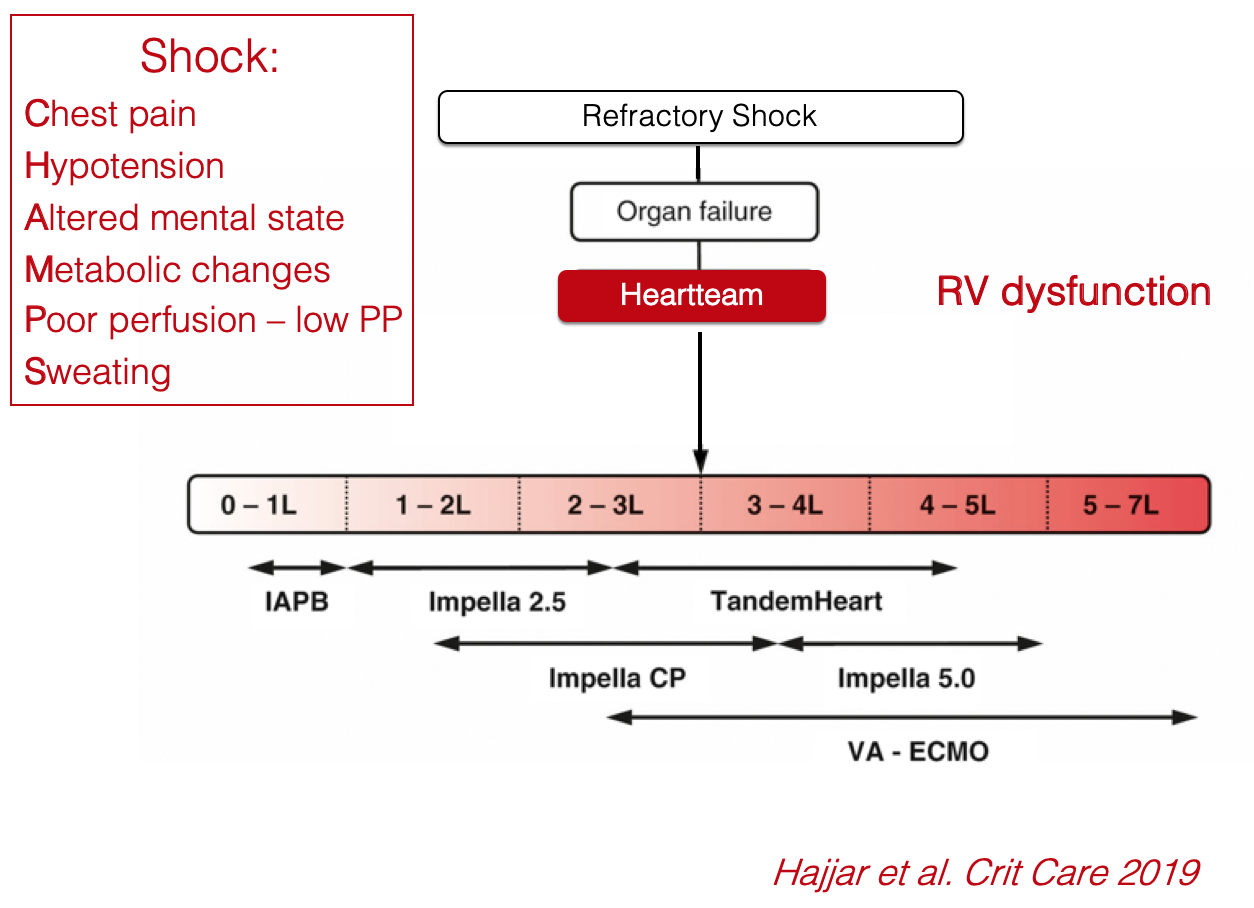
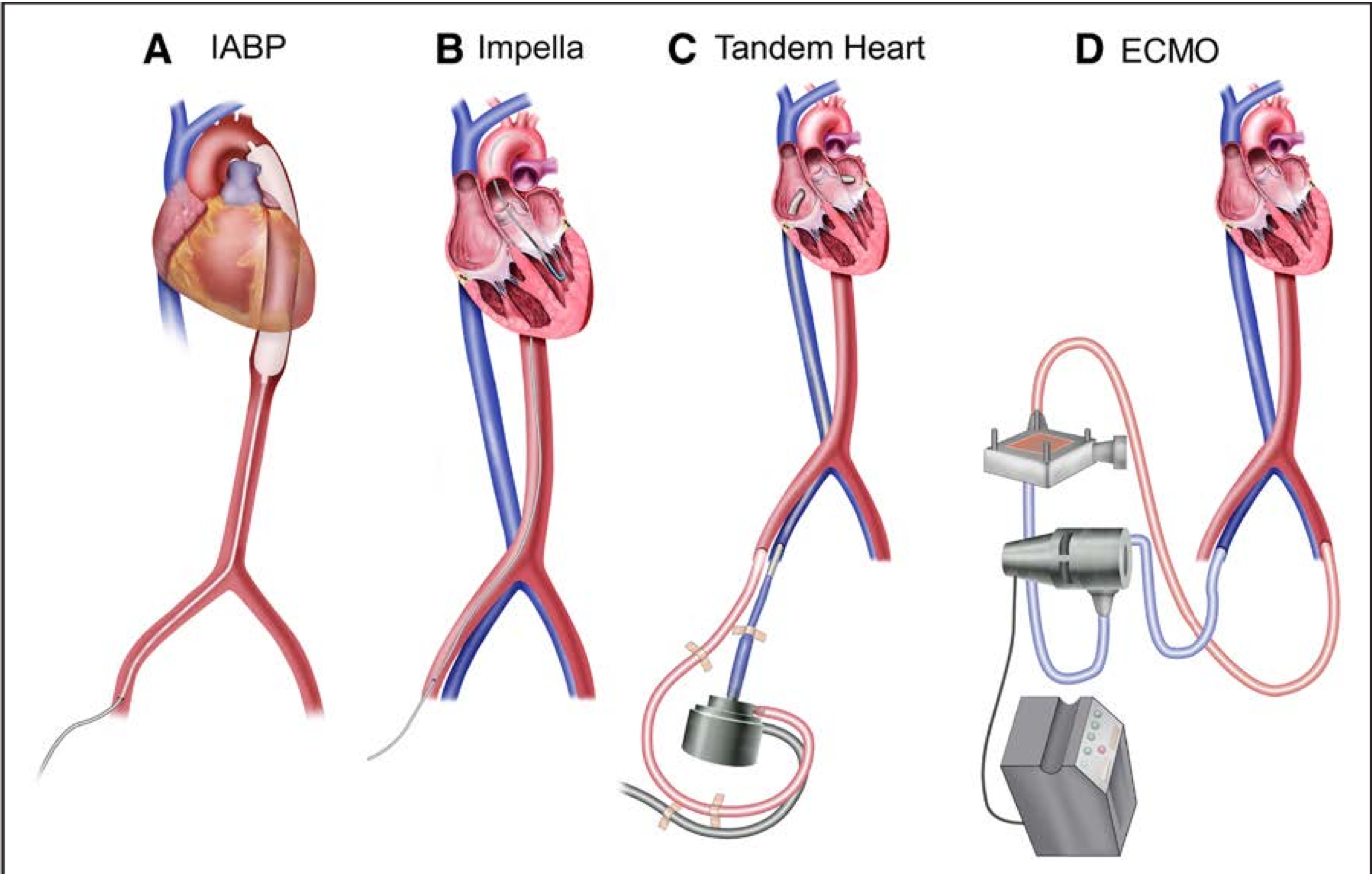
Mechanical Circulatory Support Devices for Cardiogenic Shock: State of the Art
Management of cardiogenic shock complicating myocardial infarction: an update 2019
IN CONCLUSION
Selection of the right patient at the right time
When to start and stop ECMO
Avoid Bridge to nowhere
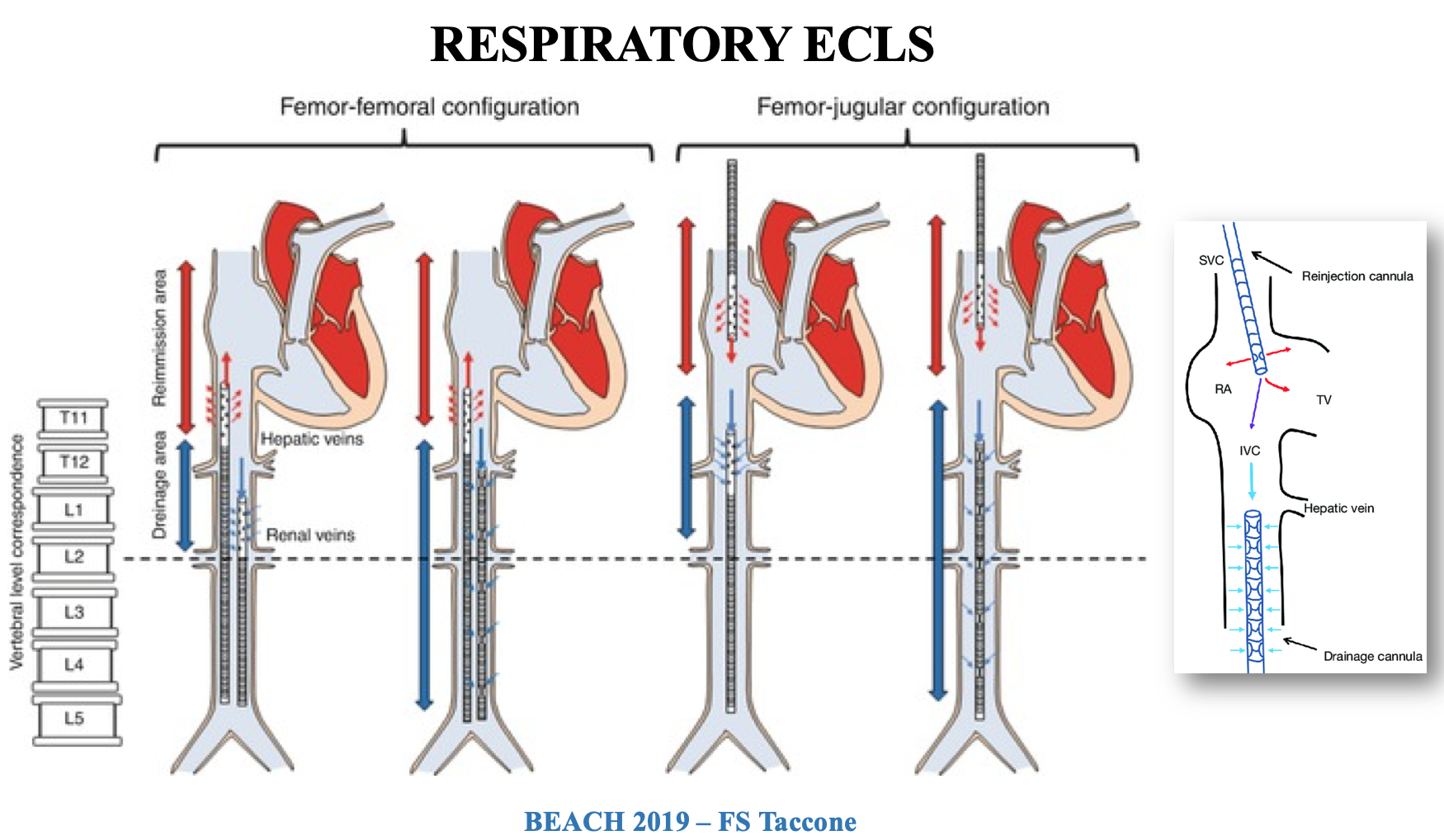
ECMO Principles and Different Modes
VV-ECMO functions as an artificial lung working in addition to the patient's own failing lungs
- To maintain gas exchanges
- To allow protective ventilation
- To allow “lung rest”
- To allow “lung recovery”
- To gain time for LTx
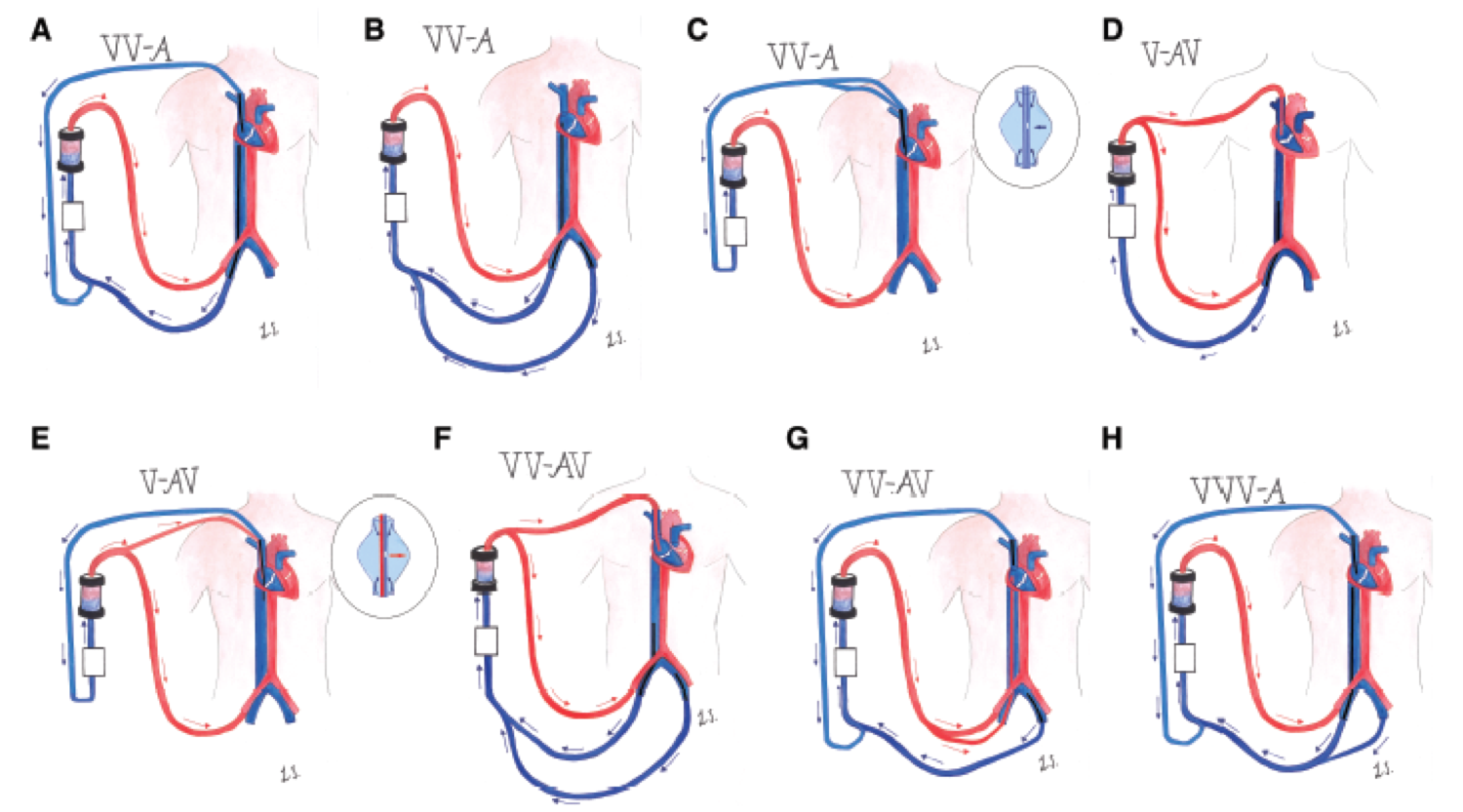
Cardiac ECMO
Multiple configurations - The ELSO Maastricht Treaty for ECLS Nomenclature: abbreviations for cannulation configuration in extracorporeal life support - a position paper of the Extracorporeal Life Support Organization
Anticoagulation and ECMO
Monitoring coagulation on ECMO
- Combination of ACT, aPTT, anti Xa with
- ATIII
- Platelet count / function
- Fibrinogen
- Viscoelastic test (How fast- how strong- for how long?)
NO SINGLE TEST may be considered adequate to guide (UFH) management