What is new in IAP measurement (#IFAD2018 #iFADmini)
Is there anything new in IAP measurement?
Determinants of IAV and IAP
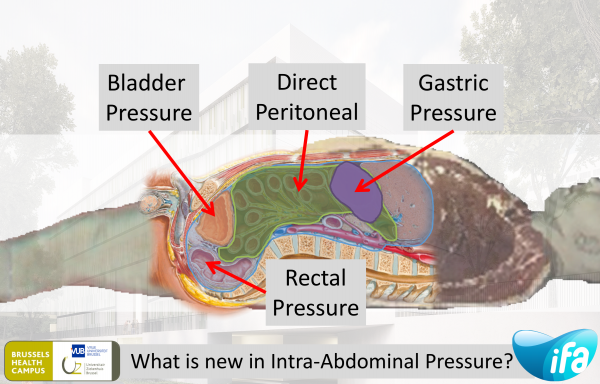
The abdominal compartment is primarily fluid in character and as such follows the law of Pascal, stating that pressures are equally transmitted throughout the entire compartment. As such IAP can be estimated via the bladder, the stomach, the rectum or directly. The relation between IAV and IAP defines abdominal compliance, a parameter that is often neglected. There are differnt ways to estimate IAP.
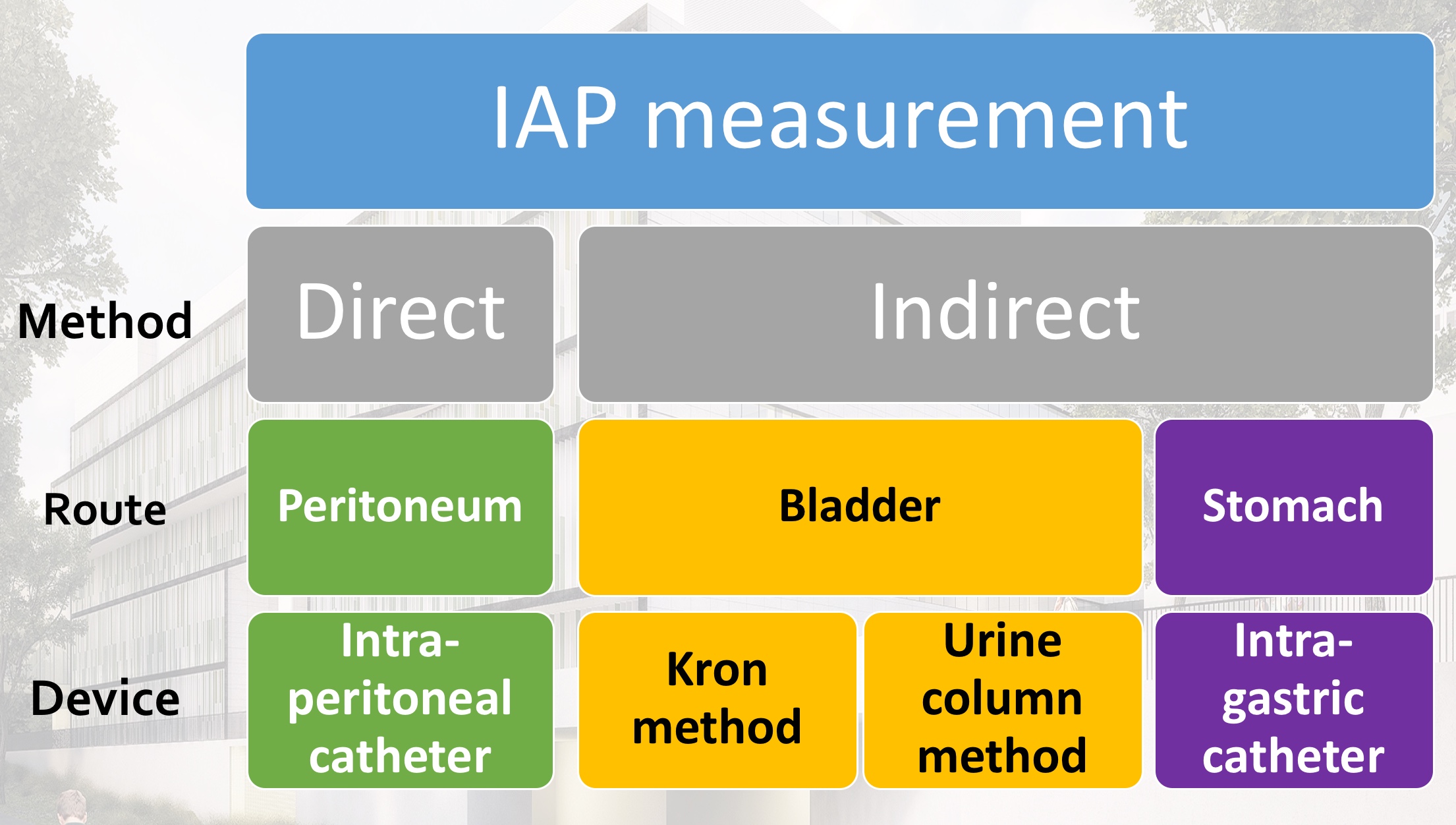
Direct IAP measurement
Direct measurement via an intraperitoneal needle or catheter is not advised in the ICU because it is invasive and carries the risk of infection, bleeding, or trauma to the bowel. It is often used as gold standard in animal research.
Noninvasive techniques
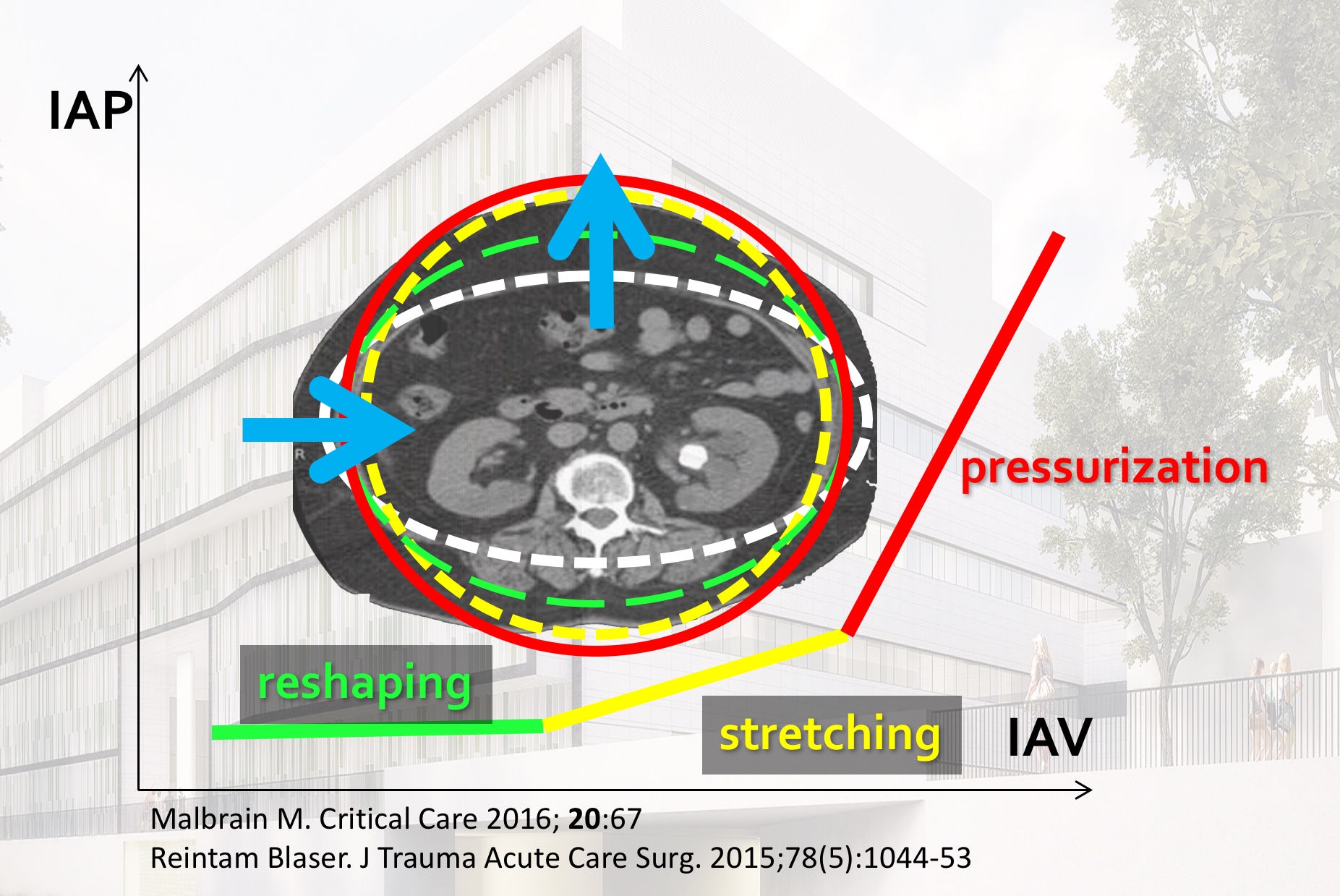
Clinical estimation is unreliable. Noninvasive techniques include estimation via ultrasound and looking at the indent of the abdominal wall by an external force (eg via tensiometer). Or by looking at the stretch on the abdominal wall (abdominal wall thickness). Normally the IAV form reshapes from ellipse to a more sphere-like shape. The latter relates to the metabolic syndrome. Therefore the presence of abdominal/visceral fat (sphere) is less favourable than subcutaneous fat (ellipse). The figure below illustrates the different phases from reshaping to stretching to pressurization.
Bladder pressure measurement
IAP is the steady-state pressure concealed within the abdominal cavity. The reference standard for intermittent IAP measurements is via the bladder with a maximal instillation volume of 25 mL of sterile saline. IAP should be expressed in mmHg and measured at end-expiration in the supine position after ensuring that abdominal muscle contractions are absent and with the transducer zeroed at the level of the midaxillary line. Normal IAP is approximately 5–7 mmHg and around 10 mmHg in critically ill adults.
Advantages continuous IAP measurement
Continuous IAP (CIAP)
- IAP trend
- Assess effect of treatment
- Look at interaction between physiologic variables (CVP, PEEP, ICP, IAP, ITP,...)
- Analyse raw data signal
Calculation abdominal perfusion pressure (APP = MAP-IAP)
- APP trend
- Better resuscitation target
- Assess effect of treatment
- Look at interaction between physiologic variables (APP, CPP, RPP...)
Automatic calculations
- Computer analysis
- Area under the curve (AUC)
- Time above a threshold (TAT)
- May be related to prognosis (in analogy to sustained increased ICP)
Assessment of polycompartment interactions
- Polycompartment syndrome (eg combined neuro + abdominal trauma)
- Organ-organ interactions (lung-heart, abdomen-brain, abdomen-lung, abdomen-heart, etc)
- Assess effect of treatment
Calculation of pressure transmission
- ATI: abdomino-thoracic index of transmission (on average 50%)
- TAI: thoraco-abdominal index of transmission
Finetuning of mechanical ventilation
- COPD (with forced expiration: endexpiratory IAP will then be greater than endinspiratory value)
- During NIV after abdominal surgery
- Asynchrony detection
- Difficult weaning assessment (failure to wean)
- Transdiaphragmatic pressure (TDP) and work-of)breathing (WOB)
Better lung recruitment and protective ventilation
- Lung protective ventilation settings
- Best PEEP = IAP
- Opening pressures = 40 + IAP/2 by 40 manoever
- P/V loops to identify safe ventilator settings
Noninvasive assessment of abdominal compliance
- RAVT (respiratory abdominal variation test)
- APV (abdominal pressure variation = delta IAP divided by mean IAP)
- Respiratory variations (Delta IAP)
Analysis of raw IAP data with filters
- IAP
- Delta IAP, APV (abdominal pressure variation)
- Heart rate
- Respiratory rate
- Relative PPV (pulse pressure variation)
- Relative SV/CO
Take Home messages
- Clinical estimation unreliable
- Measuring IAP = Knowing IAH and diagnosing ACS
- Noninvasive techniques (ultrasound) seem promising
- Continuous IAP has major advantages
- IAP and APP trend: assess effect treatment + adapt resuscitation targets
- Automatic calculations AUC and TAT for outcome prediction
- Estimation of compliance: RAVT and APV
- Transdiafragmatic pressure (IGP-Peso) ⇒ WOB
- Raw data filter: noninvasive assessment of HR, RR, PPV, relative SV
In this lecture given by @manu_malbrain during the 38th #ISICEM18 meeting held in Brussels the above mentioned concepts are explained and discussed. Why wait, just start measuring IAP now avoiding IAH and ACS and understanding the polycompartment syndrome:
Go to Video
Suggested reading
- Malbrain ML: Different techniques to measure intra-abdominal pressure (IAP): time for a critical re-appraisal. Intensive care medicine 2004, 30(3):357-371.
- Sugrue M, De Waele JJ, De Keulenaer BL, Roberts DJ, Malbrain ML: A user's guide to intra-abdominal pressure measurement. Anaesthesiol Intensive Ther 2015, 47(3):241-251.
- Malbrain ML, Peeters Y, Wise R: The neglected role of abdominal compliance in organ-organ interactions. Critical care (London, England) 2016, 20:67.
- Malbrain ML, De laet I, De Waele JJ: Continuous intra-abdominal pressure monitoring: this is the way to go! Int J Clin Prac 2008, 62(3):359-362.
- De Waele JJ, De laet I, Malbrain ML: Rational intraabdominal pressure monitoring: how to do it? Acta Clin Belg Suppl 2007, 62(1):16-25.
- Malbrain MLNG, Roberts DJ, Sugrue M, De Keulenaer BL, Ivatury R, Pelosi P, Verbrugge F, Wise R, Maes H, Mullens W: The Polycompartment Syndrome: A Concise State-of-the-Art Review. Anaesthesiol Intensive Ther 2014, 46(5):433-450.