
An overview of what has been published on fluid strategies in COVID-19, guidelines available and reflections on personal practice.
Written by Manu L.N.G Malbrain, Serene Ho, and Adrian Wong
Originally published in ICU Management https://healthmanagement.org/c/icu/issuearticle/thoughts-on-covid-19-from-the-international-fluid-academy under Open Access CC BY Licence 4.0
Introduction
The global COVID-19 pandemic has sharply focused the attention of the world onto critical care as a specialty. At the moment, there are no proven treatments for COVID-19, although several trials and case series extolling the merits of various agents have been published. As always, good intensive care practice is founded on a strong understanding of physiology and doing the basics well.
Whilst issues such as staffing, resources and ventilation strategies are undoubtedly important when considering a holistic approach to treating COVID-19, fluid management remains a cornerstone of intensive care.
Unsurprisingly, given that it is a novel virus and illness course, published data and guidelines on how best to treat patients with COVID-19 are continually evolving. The experiences and data shared by frontline colleagues in China and Italy, who have had to deal with the pandemic before the other countries were affected, are hugely invaluable. In this paper, we summarise what has been published on fluid strategies in COVID-19, guidelines available and provide some reflections on personal practice. Importantly we ask colleagues to rally around this important issue and review their own practice with regards to fluid therapy.
What do we Know?
There is little doubt that fluid therapy, either too much or too little, can adversely affect patient outcome (Malbrain 2018). As a novel disease, the general principles of fluid management in critical care provides the foundation for fluid therapy in COVID-19, but the shared experiences of colleagues add to and refine this. The goals of resuscitation and management are therefore constantly evolving.
As an example, during the early stages of the COVID-19 pandemic, it was common advice to aim for a negative fluid balance. More recently, a higher than expected occurrence of acute kidney injury requiring renal replacement therapy has been observed, prompting calls for a more liberal fluid strategy.
A particular challenge is the fact that patients are presenting at different stages of their illness. Those that are admitted to hospital later in the illness may be hypovolaemic due to increased losses from fever and tachypnoea. Whilst most cases primarily present with respiratory symptoms, gastrointestinal symptoms such as vomiting and diarrhoea are not uncommon. Hence it is important to take a concise history (paying particular attention to symptom onset), clinically assess the patient and individualise therapy.
In general, a judicious fluid strategy whereby fluid is cautiously administered only after pre-load responsiveness has been assessed as preferable (Silversides, 2019). Given the incidence of myocardial dysfunction in a subset of patients (Zheng, 2020), early use of vasopressors/inotropes alongside regular assessment via echocardiography would be prudent.
What Guidelines are Available?
Several organisations and professional societies have published guidelines on the management of patients with COVID-19. With regards to fluid therapy, the core recommendations stem from the initial Surviving Sepsis Campaign guidelines along with its COVID-19 specific update (Alhazzani et al. 2020). However, no direct evidence exists for patients with COVID-19 and shock, therefore indirect evidence from critically ill patients with sepsis and ARDS was used to formulate these recommendations. A selection of these guidelines with emphasis on fluid management is summarised below.
Surviving Sepsis Campaign
The Surviving Sepsis Campaign group has suggested the following in their COVID-19 specific guidelines for acute resuscitation of adults with shock:
- Measuring dynamic parameters to assess fluid responsiveness (weak recommendation; low quality of evidence [QE]),
- Using a conservative fluid administration strategy (weak recommendation; very low QE),
- Using crystalloids in preference to colloids (strong recommendation; moderate QE),
- Balanced crystalloids preferred over unbalanced crystalloids (weak recommendation; moderate QE).
As shown, these recommendations are based on low quality evidence.
World Health Organization
World Health Organization guidelines recommend that patients with COVID-19 in respiratory failure should be treated cautiously with intravenous fluids, especially in settings with limited availability of mechanical ventilation.
- Use a conservative fluid management strategy for ARDS patients without tissue hypoperfusion.
- In resuscitation for septic shock in adults, give 250–500 mL crystalloid fluid as a rapid bolus in the first 15–30 minutes and reassess for signs of fluid overload after each bolus.
- If there is no response to fluid loading or if signs of volume overload appear, reduce or discontinue fluid administration.
- Consider dynamic indices of volume responsiveness to guide volume administration beyond initial resuscitation based on local resources and experience. These indices include passive leg raises, fluid challenges with serial stroke volume measurements, or variations in systolic pressure, pulse pressure, inferior vena cava size, or stroke volume in response to changes in intrathoracic pressure during mechanical ventilation.
- Starches are associated with an increased risk of death and acute kidney injury compared to crystalloids. The effects of gelatins are less clear, but they are more expensive than crystalloids. Hypotonic (vs isotonic) solutions are less effective at increasing intravascular volume. Surviving Sepsis also suggests albumin for resuscitation when patients require substantial amounts of crystalloids, however this conditional recommendation is based on low-quality evidence.
UK Joint Anaesthetic and Intensive Care Guidelines
- Conservative fluid management strategy in ARDS.
- In cases of significant hypotension or circulatory shock, standard circulatory assessment (fluid responsiveness, cardiac output assessment) and administration of an appropriate fluid and/or pressor (where appropriate) should occur.
- Balanced electrolyte solutions are preferred to 0.9% saline and colloids.
- While fluid overload should be avoided and more conservative administration may help improve respiratory function, this should be carefully balanced against the risk of inducing acute renal impairment.
- Care should be exercised in ‘running patients too dry’ in an effort to spare the lungs, as there are increased insensible fluid losses.
Guidance and Recommendations from the International Fluid Academy
The following are some suggestions and best practice recommendations taking into account those mentioned above.
Assessment and monitoring
- The patient’s fluid balance is assessed on admission in the hospital and on a daily basis with cumulative fluid balance calculated.
- Assessment of fluid and electrolyte requirement as part of every clinical review using a combination of clinical judgement, vital signs and chart records.
- Recent laboratory results with urea and electrolytes (at least once every 24 hours of fluid prescription).
- The use of cardiac output monitors to assess fluid responsiveness e.g. ultrasound (see below) and bioimpedance monitoring (Figure 1).
Resuscitation
- Use balanced crystalloids (e.g. plasmalyte).
- Do not use starch solutions or gelatins.
- Do not use albumin in the early stages.
- For patients in need of fluid resuscitation:
- Identify the cause of fluid deficit.
- Assess for presence of shock or hypoperfusion.
- Assess fluid responsiveness (see further).
- Give a bolus of 4 mL/kg of balanced crystalloids over 10-15 minutes.
- Fluid responsiveness is assessed before and after fluid administration with functional haemodynamics e.g. pulse pressure variation (PPV) or other tests e.g. passive leg raise test or end-expiratory occlusion test, or a combination.
- Mean arterial pressure and cardiac output are continuously monitored.
- Early initiation of vasopressors: noradrenaline at low dose 0.05mcg/kg/min.
- Consider the addition of vasopressin/argipressin when noradrenaline dose exceeds 0.5 mcg/kg/min
- Assess for the presence of fluid overload (i.e. 10% increase in body weight or volume excess from baseline).
- Start de-resuscitation whenever possible.
- Replace serum albumin to approximately 30 g/L with albumin 20%.
- Use combination therapy of diuretics: loop + spironolactone + acetazolamide (when BE > 5) + indapamide (in cases of hypernatraemia).
- Consider ultrafiltration (even in the absence of acute kidney injury) when diuretics fail to achieve zero fluid balance.
Maintenance fluids
- Do not administer maintenance fluids in patients who are eating and drinking sufficiently.
- Use balanced solutions (e.g. Glucion 5% or Maintelyte).
- In patients requiring IV fluids for routine maintenance alone, the initial prescription should be restricted to:
- 25–30 mL/kg/day (1 mL/kg/hr) of water
- approximately 1 mmol/kg/day of potassium (K+)
- approximately 1-1.5 mmol/kg/day of sodium (Na+)
- approximately 1 mmol/kg/day of chloride (Cl-)
- approximately 50–100 g/day (1-1.5 g/kg/day) of glucose to limit starvation ketosis
- The amount of fluid intake via other sources should be subtracted from the basic maintenance need of 1ml/kg/hr e.g. nutrition and fluid creep (see below).
Fluid creep
- All sources of fluids administered need to be detailed: crystalloids, colloids, blood products, enteral and parenteral nutritional products, intravenous medication and oral intake (water, tea, soup, etc.)
- Precise data on the concentrated electrolytes added to these fluids or administered separately need to be documented.
- Fluid creep is defined as the sum of the volumes of these electrolytes, the small volumes to keep venous lines open (saline or glucose 5%) and the total volume used as a vehicle for medication.
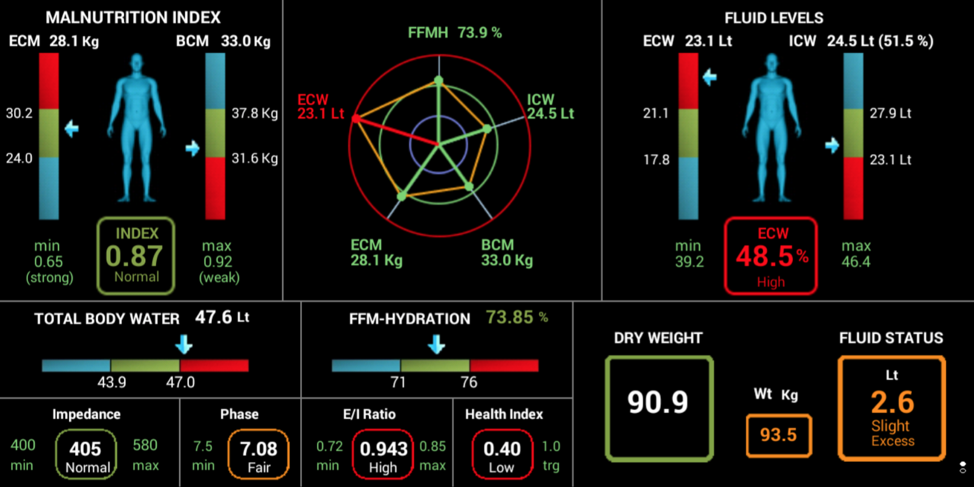
Figure 1. Sample screenshot with results obtained via full body, multifrequency bioelectrical impedance analysis (BIA) with touch i8 device (Maltron, UK) showing a volume excess of 2.6 litres and an increased ECW : ICW ratio of 0.943 indicating capillary leak. The patient’s fluid composition is monitored with BIA separating intra- and extracellular water and estimating the volume excess (Ref https://pubmed.ncbi.nlm.nih.gov/31808061/).
The Role of Ultrasound
Although numerous monitoring devices are available to help the clinician formulate management plans, ultrasound ranks as one of the most versatile diagnostic and monitoring tools particularly when applied to fluid therapy. Its portability and therefore ease of use at the bedside is desirable in the presence of strict infection control measures. No other singular device is able to non-invasively evaluate and assess response to therapy for the cardiovascular, respiratory and renal systems. Indeed, critical care ultrasound has always enjoyed the benefit of providing a holistic, integrated approach to patient care, but it is during the COVID-19 pandemic that it has really come into its own.
A non-exhaustive summary of the potential ultrasonographic assessments that can be performed are listed below.
|
System |
Identifiable structures |
Measurable parameters |
Potential indication in COVID-19 |
|
Airway |
Tracheal rings Cricothyroid membrane Thyroid cartilage Hyoid bone |
Distance to structures Diameter of trachea Presence of edema or external compression |
Plan for difficult intubation and extubation |
|
Thoracic |
A-lines B-lines Consolidation Collapse Effusion Diaphragm |
Number of B-lines Volume of effusion, depth to effusion Extent of pneumothorax (lung sliding, lung-point) Diaphragmatic function |
Assess degree of lung involvement Diagnose any concurrent conditions |
|
Cardiac |
Right atrium and ventricle Left atrium and ventricle AV valves Pulmonary valves Aortic valves Inferior vena cava |
Size and dimension Valvular pathologies Systolic and diastolic dysfunction Presence of mass/vegetation Regional wall motion abnormalities |
Assess cardiovascular function Assess response to therapy e.g. fluid bolus |
|
Abdominal |
Free fluid e.g. ascites, blood Aorta Inferior vena cava Gastric content |
Size of organs Size of vascular structures Doppler analysis of vascular flow to organs Volume of free fluid, depth to free fluid Calculation of gastric residual volume (GRV) Inferior vena cava collapsibility index (IVVCI) |
Assess cause of liver dysfunction Part of haemodynamic assessment |
|
Renal |
Kidneys Ureter Bladder |
Size of kidneys Doppler analysis of vascular flow to kidneys (renal resistive index) Volume of bladder |
Assess cause of renal dysfunction |
|
Vascular |
Thrombosis (clot visualisation) Dissection |
Doppler analysis of vasculature Compression of veins |
Aid vascular catheter placement Diagnose venous thrombosis |
Table 1. Potential ultrasonographic assessments.
Fluid Stewardship - Knowing What we are Doing
As with antibiotic stewardship, fluid stewardship can improve the quality of clinical care. Typically, this would involve a stepwise approach in assessing current practice and outcomes - a clear view of current practice will highlight the areas where we are performing well, and those that are lacking, so as to provide a basis for meaningful change (Malbrain 2018). Patients should have an IV fluid management plan, including a fluid and electrolyte prescription over the next 24 hours agreed by the intensive care team, taking into account clinical and laboratory findings, supplemented by the appropriate imaging e.g. ultrasound. These can be summarised by the ‘Rules of Fours’ in Table 2.
|
4 Questions |
4 Indications |
4 Ds |
4 Stages |
4 Hits |
|
When to start IV fluids When to stop IV fluids When to start removing fluids When to stop removing fluids |
Resuscitation Maintenance Replacement Nutrition |
Drug Dose Duration De-escalation |
Resuscitation Optimisation Stabilisation Evacuation (de-escalation) |
1st HIT: initial insult (eg COVID with sepsis) 2nd HIT: ischemia and reperfusion 3rd HIT: fluid accumulation and GIPS (global increased permeability syndrome) 4th HIT: hypoperfusion during de-resuscitation |
Table 2. The rules of fours
Of course, there will be colleagues who argue that trying to collect data on fluid prescription during an international pandemic is pointless or inconvenient. However, we maintain that there are several arguments against this.
Firstly, there has been, undoubtedly, significant change to our clinical practice due to changes in the logistics of critical care delivery. New clinical areas have been added or converted to care for critically ill patients. To staff these new critical care/high-dependency areas, healthcare professionals from outside of critical care are being redeployed, and require training and education. Whilst data collection requires the investment of time and energy, this time of upheaval is all the more reason for accurate documentation and data analysis so as to ensure that various aspects of patient care can be visualised on a larger scale.
Furthermore, we have seldom been more acutely aware of the limitations of medical resources - healthcare professionals, personal protective equipment, machines for mechanical ventilation and haemofiltration, right down to the drugs we consider to be basic essentials in critical care. The understanding of illness processes and patient outcomes, as well as how our interventions affect these, will enable us to streamline and rationalise our utilisation of precious resources so as to maximise their benefits for our patients whilst avoiding undue harm. This principle is similarly applicable to the experimental use of existing medications in COVID-19 including anti-virals, anti-malarials etc, and is particularly relevant in the case of hydroxychloroquine where stock shortages will likely impact upon the patients requiring this drug for its prescribed usage.
Last but not least, given the extensive spread of COVID-19, there has been a dramatic shift in the patient population in many hospitals, with a preponderance of COVID-19 cases. There is the potential for a multitude of lessons we can learn in a very short space of time, from the management of these patients. These will help us refine our treatment plans for subsequent waves of infection, and could be extrapolated to other epidemics in future.
Ultimately when the pandemic is over, the collection of such data would allow for us to reflect, review and improve on clinical practice.
Conclusion
Fluid administration and management are one of the fundamental practices of intensive care. The principles of good fluid practice are built upon the foundations of a firm understanding of the underlying pathophysiological process. COVID-19 is a novel illness and presents unique challenges not just to clinical practice but the entire healthcare system.
We would argue that the principles of fluid stewardship have never been more important in clinical practice than now. The unique challenges present an opportunity to improve the quality of care delivered not just for the current pandemic but for future ones.
Just because it is difficult, doesn’t mean it is not worth the effort. We are dealing with an unprecedented healthcare event in modern times, with mind-boggling technology and the ability to swiftly disseminate information on our side. Whether we handle it ‘the old way’ or embrace all the tools and collaborative opportunities available to us may well decide how this pandemic goes down in history. We firmly believe in the latter approach.
Conflict of Interest
Manu Malbrain is the founder of the International Fluid Academy. Serene Ho and Adrian Wong are members.
Key Points
- The general principles of fluid management in critical care provides the foundation for fluid therapy in COVID-19.
- During the early stages of the COVID-19 pandemic, it was common advice to aim for a negative fluid balance but more recently there have been calls for a more liberal fluid strategy.
- It is important to take a concise history, clinically assess the patient and individualise therapy.
- Several guidelines have been published on the management of patients with COVID-19 including the Surviving Sepsis Campaign Group Guidelines, the WHO and the UK Joint Anaesthetic and Intensive Care Guidelines.
- Ultrasound ranks as one of the most versatile diagnostic and monitoring tools particularly when applied to fluid therapy.
- As we continue to learn, we can refine our treatment plans for subsequent waves of infection, which could be extrapolated to other epidemics in future.
About the IFA
The International Fluid Academy was founded in 2011 with the goals to foster education and promote research on fluid management and monitoring in critically ill patients, and thereby improve the survival of critically ill patients by bringing together physicians, nurses, and others from a variety of clinical disciplines. It aimed to improve and standardise care and outcome of critically ill patients with an emphasis on fluids, fluid management, monitoring and organ support by collaborative research projects, surveys, guideline development, joint data registration and international exchange of health care workers and researchers. We invite the reader to follow @Fluid_Academy and to check this website (www.fluidacademy.org) for more information on fluid management and haemodynamic monitoring (under FOAM resources).